- Forget Me Not
- Posts
- The Evolution of Caring: what bereavement care looked like in every decade
The Evolution of Caring: what bereavement care looked like in every decade
Every week, we deliver evidence-based strategies for modern perinatal bereavement care. Written by Jay CRNA, MS, specializing in obstetrical anesthesia, and Trina, a bereavement expert, both who have experienced loss.
Trina Parkin
January 01, 2026 • Read time: 7 minutes
In Today’s Issue:
🔗 The best resources I found this week
📖 Deep dive: The Evolution of Caring: what bereavement care looked like in every decadeDifferent Cultures and Ethnicities
Know a co-worker who would benefit from this newsletter? Subscribe here
Want to learn how to get Forget Me Not Boxes in your hospital? Reply “Bereavement boxes”

🔗 The Best Resources I Found This Week
📜 Historic Traditions for Mourning the Death of a Child
Different cultures have always found ways—some structured, some restrictive—to acknowledge the death of a baby or child. (Listverse)
📷 Post-Mortem Photography and the History of Infant Mourning
Victorian post-mortem photography wasn’t about morbidity—it was about remembrance in a time when infant death was common. (Smithsonian Magazine)
🏥 How Modern Medicine Changed the Way We Grieve Infant Death
As death moved from the home to the hospital, rituals changed—and often disappeared. This piece examines how medicalization reshaped grief, including infant and child death, and what was lost along the way.
Read the full article here (Wellcome Collection)
📖 Deep Dive
The Evolution of Caring: what bereavement care looked like in every decade
The way we care for grieving parents hasn’t always looked the way it does today. Across cultures and centuries, societies have tried to answer the same question: How much grief is allowed, and for how long? Some answers were shaped by philosophy, some by fear, and others by medicine catching up to human experience. This timeline traces the evolution of bereavement care—not to criticize earlier eras, but to understand why today’s practices matter so deeply.
Ancient China Limited Mourning for Babies Based on Age (Pre-20th Century)
In ancient China, infant death was governed by strict cultural rules about who was allowed to grieve—and for how long. If a baby died before three months of life, parents were not permitted a formal mourning period at all. For children who lived longer, grief was rationed: parents were allowed one day of mourning for each month the child had lived. A six-month-old baby meant six days of sanctioned grief, and no more.
The reasoning was philosophical rather than cold. Children under roughly eight years old were believed not to have fully entered social life, meaning their deaths—while sad—were not considered tragedies requiring prolonged ritual. Parents were forbidden from wearing official white mourning robes or spending money on elaborate funerals.
This approach stands in stark contrast to Western traditions of the same era, which surrounded infant death with heavy ritual. Both cultures were responding to heartbreak—but expressing it through very different rules about visibility and restraint.
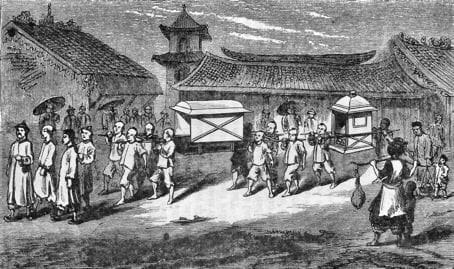
Historic illustration depicting traditional Chinese mourning practices.
Victorian England Used White Door Ribbons to Signal a Child’s Death (Mid-1800s)
In Victorian England, grief was meant to be seen. Families announced a death by hanging crepe and ribbon on the front door, turning the home itself into a signal to the community.
Color mattered. White ribbons were used when the person who died was a child or unmarried young person, while black—or black trimmed with white—marked the death of an adult. Neighbors could tell at a glance who had died, their age, and how to approach the household.
This system functioned as a quiet social code. It told people when to bring food, lower their voices, or simply show up. Mourning wasn’t private or internal—it was collective, expected, and structured.
For families who lost babies, the ribbon was often the only public acknowledgment that the child had lived at all.

Mourning Wreath, Doorway, Avenue C, New York City, Walker Evans, 1941,

Victorian-era illustration showing mourning crepe and ribbon displayed on a home.
Victorian Families Commissioned Post-Mortem Photos of Infants (Late 1800s)
In the late 19th century, photography offered grieving parents something rare: permanence. Families frequently commissioned post-mortem photographs of infants, carefully posed to appear as if sleeping.
Often, the baby was held upright by the mother, who remained hidden behind dark fabric or positioned just outside the frame. These images weren’t considered unsettling at the time. They were often the only photograph ever taken of the child, especially in an era when infant mortality was common and photography was expensive.
For parents, the photo served as proof of existence. A tangible record that this baby was real, loved, and mourned.
What looks unfamiliar to modern eyes functioned then as a deeply human attempt to hold on to something that vanished too quickly.

Victorian post-mortem photograph style, with infant posed as sleeping.
Around 1900, Infant Death Was Common Enough to Shape Daily Life
At the turn of the 20th century, infant death was not rare—it was expected. Estimates suggest that 150–165 out of every 1,000 babies born in the United States around 1900 did not survive their first year. Even by 1915, when national data became available, infant mortality still hovered around 100 per 1,000 live births.
These numbers shaped behavior. Families often kept burial clothing at home. Funeral homes had standard pricing for infant services. Communities had well-rehearsed rituals for baby deaths because nearly everyone encountered one.
This context helps explain why mourning practices could feel restrained or pragmatic. Loss was constant. Grief had to coexist with survival.


Early public health chart illustrating infant mortality rates
Hospitals Replaced Homes as the Place of Death (1930s–1950s)
Between the 1930s and 1950s, birth and death moved out of the home and into hospitals. What had once been family-centered events became medical ones, governed by efficiency, protocols, and professional authority.
This shift dramatically altered bereavement. Hospitals prioritized infection control, workflow, and emotional “containment.” Death became something to manage quietly, behind closed doors.
This institutionalization laid the groundwork for later practices of sedation, separation, and silence following stillbirth. What families lost was not care—but control.


Mid-century hospital maternity ward.
Mothers Were Sedated and Fathers Were Excluded After Stillbirth (1940s–1960s)
From the 1940s through the 1960s, obstetric care routinely relied on maternal sedation and paternal exclusion following stillbirth. Mothers were often given scopolamine, barbiturates, or opiates during labor, with sedation frequently continued afterward to limit emotional distress and memory formation.
Fathers were typically not allowed in delivery rooms, rarely permitted to see the baby, and sometimes advised not to discuss the death with the mother “for her own good.”
The belief was simple: avoidance would prevent suffering. Later research would show the opposite—separation often deepened long-term grief rather than protecting families from it.
A 1950s hospital delivery room and sterile tools to be utilized during birth.
The 1970s Challenged Separation and Changed Bereavement Care
By the 1970s, infant mortality had declined significantly, but understanding of grief entered a crisis point. Researchers John Kennell and Marshall Klaus, building on attachment theory, studied what happened when mothers were separated from deceased infants versus allowed contact.
Their findings were clear: separation, sedation, and discouraging grief worsened psychological outcomes. Attachment began during pregnancy, not after birth. Preventing contact did not prevent grief—it complicated it.
This research directly contradicted decades of medical practice and sparked change. Hospitals slowly began offering parents the option to see, hold, name, and remember their baby. Memory-making was no longer seen as dangerous—it became therapeutic.
The 1980s Formalized Bereavement Care as Medicine Advanced
By the 1980s, neonatal intensive care had transformed infant survival—but also complicated end-of-life care. As more babies lived longer, decisions around withdrawing support, comfort care, and dying became more complex.
During this decade, bereavement care became increasingly formalized. Hospitals introduced footprints, photographs, and keepsakes. Chaplains and social workers joined care teams. Parents were more routinely offered time with their baby.
SIDS also dominated postneonatal death, triggering mandatory investigations and autopsies. While medically necessary, this process layered trauma onto grief—prompting the rise of specialized support organizations and improved communication training for professionals.


Widow Support Group, Tri-Cities Chaplaincy
Everly’s Law Recognized Stillbirth as the Death of a Child (Texas, 2021)
In 2021, Texas passed Everly’s Law, a milestone that quietly corrected decades of institutional language around stillbirth. The law allows parents who experience stillbirth at or after 20 weeks to request a Certificate of Birth Resulting in Stillbirth, formally acknowledging that their baby existed and died.
Before this, many parents left the hospital with no official document bearing their baby’s name—only medical records and silence. Everly’s Law changed that by recognizing stillbirth as the death of a baby, not simply a failed pregnancy outcome.
The law was named after Everly, a baby whose parents advocated publicly for recognition after realizing how isolating it felt to have no legal acknowledgment of her life. While symbolic, the impact is real: documentation matters in grief. It validates parenthood, affirms loss, and signals that the healthcare system sees what happened.
Everly’s Law reflects a broader shift toward dignity, language, and agency in bereavement care—but also highlights how recently these conversations have entered policy.
Footnotes & Sources
Jalland, P. (1996). Death in the Victorian Family. Oxford University Press.
— Definitive historical analysis of mourning customs, including child death rituals and symbolism.Curl, J. S. (2000). The Victorian Celebration of Death. Sutton Publishing.
— Documents mourning dress, door symbols, and public grief practices.Batchen, G. (2004). Forget Me Not: Photography and Remembrance. Princeton Architectural Press.
— Primary scholarly source on post-mortem photography and “hidden mother” images.Centers for Disease Control and Prevention. (1999). Achievements in Public Health, 1900–1999: Healthier Mothers and Babies.
— Provides infant mortality data and historical trends.Aries, P. (1981). The Hour of Our Death. Alfred A. Knopf.
— Foundational work on the medicalization of death and the shift from home to hospital.Leavitt, J. W. (2009). Make Room for Daddy. Johns Hopkins University Press.
— Details paternal exclusion and maternal sedation in mid-20th-century obstetrics.Kennell, J. H., & Klaus, M. H. (1976, 1993). Parent-Infant Bonding. Mosby.
— Seminal research demonstrating harm caused by separation after infant death.Bowlby, J. (1969). Attachment and Loss, Vol. 1. Basic Books.
— Theoretical foundation establishing attachment during pregnancy.National Institutes of Health. (1969). Proceedings of the SIDS Consensus Conference.
— Established SIDS as a diagnostic category.CDC National Center for Health Statistics. (1980–1990). Infant Mortality Reports.
— Tracks neonatal and postneonatal mortality trends and disparities.Texas Health & Safety Code §192.002 (2021). Everly’s Law.
— Legal recognition of stillbirth certificates in Texas.Limbo, R., et al. (2017). When a Baby Dies: Evidence-Based Care for Bereaved Parents.
Journal of Obstetric, Gynecologic & Neonatal Nursing.
— Reviews historical practices and modern best practices in perinatal bereavement.
👋 That’s a Wrap!
Before you go: Here are ways we can help your hospital
Education: Please share our newsletter with your co-workers. Our priority is empowering nurses with the tools to support patients with modern, evidence-based bereavement education.
Bereavement boxes: Our bereavement boxes were designed out of a need for a modern high quality solution for families suffering from miscarriage, stillborn, or infant death.
Reply to this email “Sample” to get a free sample sent to your hospital.

What we prioritize:
Tools for hospitals to create a bereavement experience for families to begin their grief journey
Educating nurses with modern bereavement standards and continuing education.
Helping hospitals build a foundation of trust and support, so bereaved families feel seen and cared for—now and in the years to come.
These boxes were born out of our own personal losses, including Jay’s (CEO) 15 years of experience working in labor and delivery as a CRNA and witnessing time and again how the hospital experience can profoundly shape a family’s grief journey, for better or for worse.
Until next week,
Trina and Jay
Co-founders of Forget Me Not
